Three-Part Series · Dermatology
The Science of Acne: Biology & Aftermath
Acne affects more than 85% of people at some point in their lives. Yet for all its prevalence, what happens beneath the skin remains widely misunderstood.
- 5 min read
- Evidence-based
- Parts 1 · 2 · 3
What Is Acne?
Understanding the biology beneath the breakout.
A Disease of the Follicle
Acne is a chronic inflammatory disease of the pilosebaceous unit — the hair follicle and its attached sebaceous (oil) gland. It is not caused by dirty skin or poor hygiene. It arises from four interconnected biological factors working against you simultaneously.
- Excess sebum production
- Clogged follicles
- Bacterial overgrowth
- Immune-driven inflammation
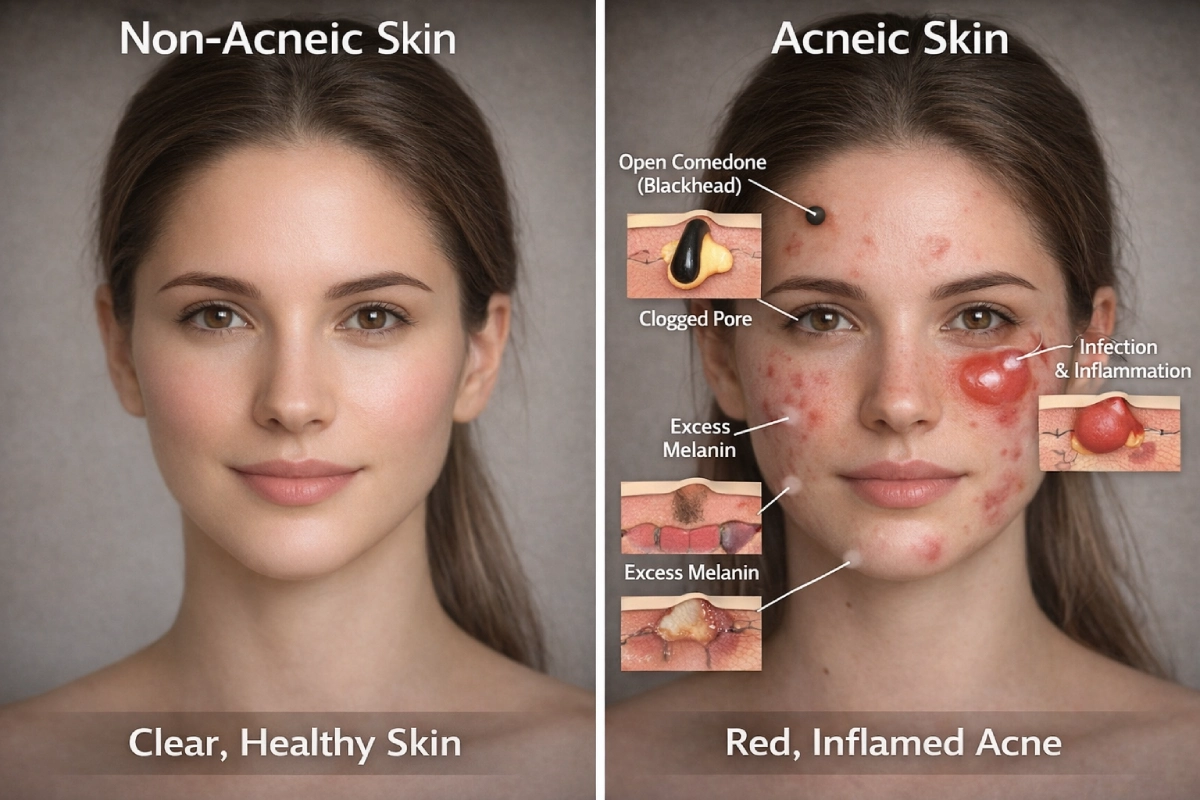
The sebaceous glands produce sebum, a waxy oil that normally lubricates the skin. When the gland overproduces — often triggered by hormonal shifts during puberty, the menstrual cycle, or stress — sebum backs up. Dead skin cells that would otherwise shed naturally stick together inside the follicle, forming a plug at the opening.
This plug is called a comedone. A closed comedone is a whitehead — sealed beneath the skin surface. An open comedone is a blackhead — exposed to air, where the tip oxidizes and turns dark. Blackheads are not dirty pores. They are simply chemistry.
Acne affects more than 85% of people at some point in their lives. Yet for all its prevalence, what happens beneath the skin remains widely misunderstood. This three-part series breaks down the science of acne, what it leaves behind, and why skin tone changes everything.
When the Immune System Gets Involved
Inside a blocked follicle, a bacterium called Cutibacterium acnes (formerly Propionibacterium acnes) thrives. It is a normal resident of healthy skin, but in the oxygen-deprived, sebum-rich environment of a blocked pore, it multiplies rapidly.
The immune system detects this overgrowth and mounts a response — dispatching white blood cells that trigger swelling, heat, and redness. This is the inflammation behind papules, pustules, nodules, and cysts. The deeper and more prolonged the immune response, the more tissue damage occurs beneath the surface.
Not all acne is inflamed. Blackheads and whiteheads are non-inflammatory comedones. Pimples, nodules, and cysts involve immune activation — and it is inflammatory acne that leaves the most significant marks.
Types of Acne Lesions
Comedones
Non-inflammatory — Whiteheads and blackheads. No immune involvement.
Papules
Small, raised, red bumps. Early inflammatory stage.
Pustules
Papules with visible pus. More pronounced inflammation.
Nodules
Large, deep, painful. Significant risk of scarring.
Cysts
Fluid-filled, the most severe form. Highest scarring risk.
Triggers and Contributing Factors
Genetics play the largest role — if both parents experienced significant acne, their children are much more likely to as well. Hormonal fluctuations (androgens stimulate sebum production), certain medications, dietary factors including high-glycemic foods and dairy in some individuals, and external irritants or occlusive skincare products can all exacerbate or trigger breakouts.
Stress does not cause acne directly, but it activates the adrenal glands to produce androgens, which accelerate sebum production. Stress also impairs the skin’s barrier function and delays healing — meaning breakouts under stress are often both more frequent and slower to resolve.
What Acne Leaves Behind
What Acne Leaves Behind
Dark spots, redness, and scars — and why they're not all the same.
When a breakout resolves, the lesion disappears — but its aftermath can persist for weeks, months, or even years. There are three distinct types of post-acne marks, and they require very different approaches to treat. Conflating them is one of the most common — and costly — mistakes in skincare.
Post-Inflammatory Hyperpigmentation (PIH)
PIH is the flat, dark spot or patch that lingers after an inflammatory acne lesion heals. It is not a scar. There is no structural skin damage, no change to the dermis. Instead, it is a pigmentation response: the skin’s melanocytes — cells that produce color — become overactive during inflammation and deposit excess melanin into the surrounding tissue.
PIH can be epidermal (closer to the surface, appears brown, more treatable) or dermal (deeper, appears gray or bluish-gray, more stubborn). Sun exposure significantly darkens both types. This is why SPF is not optional for anyone managing post-acne marks — without it, PIH that might fade in four months can persist for over a year.

Melanin inhibitors combined with cell turnover agents and consistent, daily broad-spectrum SPF.
Niacinamide
Azelaic Acid
Kojic Acid
Vitamin C
Retinoids
Alpha Hydroxy Acids
SPF daily
Post-Inflammatory Erythema (PIE)
PIE is the pink or red flat mark that remains after inflammatory acne — most visible on lighter skin tones. Unlike PIH, PIE is a vascular phenomenon. The inflammation that accompanied the pimple damaged tiny capillaries in the upper dermis. These vessels remain dilated or damaged, creating the persistent reddish discoloration.
PIE can be distinguished from PIH by a simple test: press a clear glass or fingernail against the mark. PIE will temporarily blanch (turn white), because you’re compressing the blood vessels. PIH does not blanch — it’s pigment, not blood.
Vascular-targeting therapies. PIE does not respond well to melanin-targeting treatments.
Pulsed-Dye Laser
Intense Pulsed Light (IPL)
Niacinamide
Centella Asiatica
Acne Scars
True acne scars involve structural damage to the dermis. When severe or prolonged inflammation destroys collagen, the skin cannot fully repair itself to its original architecture. Unlike PIH and PIE, acne scars do not fade on their own — they require targeted treatment.
Icepick Scars
Narrow, deep, like a puncture wound. Most difficult to treat — they extend into the deep dermis.
Boxcar Scars
Broad depressions with defined, sharp edges. Respond well to resurfacing.
Rolling Scars
Undulating, wavy texture caused by fibrous bands tethering skin downward. Subcision is often needed.
Hypertrophic Scars
The repair process overshoots, depositing excess collagen. Remain within the original wound boundary.
Keloid Scars
Extend beyond the wound boundary, can be itchy or painful, and are prone to recurrence. The risk is significantly higher in people with deeper skin tones.
Collagen damage is cumulative and permanent. Early, aggressive acne treatment prevents the inflammation that causes scars in the first place — which is always more effective than treating established scarring.
Acne & Skin of Color
Acne & Skin of Color
Why the aftermath looks different — and why that matters for treatment.
Acne is universal. Its consequences are not. For people with medium to deep skin tones — spanning Fitzpatrick types IV through VI — the aftermath of acne is often more visible, more persistent, and more distressing than the breakout itself. Yet dermatology has historically been built on lighter skin, and the gap in research, training, and clinical recognition has real consequences for patients.
The Melanin Factor
Skin of color contains melanocytes that are larger, more active, and more reactive to inflammation than those in lighter skin. Any insult to the skin — a breakout, a popped pimple, even overly aggressive treatment — can trigger a disproportionate melanin response. This is not a flaw; it is an evolutionary adaptation. But in the context of acne, it means PIH develops more easily, runs darker, and resolves far more slowly.
Where a person with lighter skin might see a pink mark fade within a few weeks, a person with a deeper skin tone can live with a dark brown or grayish patch for one to three years — even after the underlying acne is fully controlled. The emotional weight of this is significant.
Studies consistently show that patients with skin of color rate their post-acne hyperpigmentation as more distressing than the active acne itself.
PIH prevention is as important as acne treatment in patients with skin of color. Clinicians should discuss hyperpigmentation management at the same time as acne treatment — not as an afterthought.

Keloid and Hypertrophic Scarring
People of African, Asian, and Hispanic descent have a significantly higher genetic predisposition to keloid formation. On the face and chest — common sites for acne — keloids are not merely cosmetic. They can cause itching, pain, and restricted movement. Treatment is notoriously difficult: intralesional corticosteroids, silicone gels, and laser therapies can reduce them, but recurrence is common. Prevention through early and effective acne management is far more impactful than treating established keloids.
The Visibility Problem in Clinical Settings
Redness — erythema — is a standard clinical marker of acne severity. It is how clinicians assess inflammation, grade lesions, and decide on treatment. In patients with deeper skin tones, erythema is often not visible. The inflammation is present and often just as severe, but the clinical signal is masked. This has led to systematic underestimation of acne severity in patients with skin of color.
The downstream effects are measurable. Research has found that patients with skin of color are less likely to be referred to dermatologists, less likely to receive prescription-strength treatment, and more likely to experience delays in care. These delays compound: more sustained inflammation means more collagen damage, more PIH, and more scarring.
How Acne Aftermath Differs: A Side-by-Side View
| Feature | Lighter Skin Tones (I–III) | Deeper Skin Tones (IV–VI) |
|---|---|---|
| Primary aftermark | Post-inflammatory erythema (redness) | Post-inflammatory hyperpigmentation (dark spots) |
| PIH severity | Milder, resolves faster | More intense, slower to fade — often months to years |
| Keloid risk | Lower | Higher — especially African & Asian ancestry |
| Redness visibility | High — easy clinical marker | Low — inflammation often masked by pigment |
| Treatment nuance | Retinoids, vascular lasers, benzoyl peroxide generally well tolerated | Hyperpigmentation-safe actives critical; aggressive treatments can worsen PIH |
Treatment Considerations for Skin of Color
Not all standard acne treatments are equally appropriate across skin tones. The priority is to control acne while minimizing the risk of triggering additional hyperpigmentation from treatment itself.
Niacinamide
Reduces melanin transfer to skin cells, calms inflammation, and strengthens the barrier. Well-tolerated across all skin tones.
Retinoids
Effective for both acne and PIH but can cause initial irritation that worsens hyperpigmentation if introduced too aggressively. Start low and slow.
Benzoyl Peroxide
Effective antibacterial, but high concentrations can be drying and irritating, potentially triggering PIH. Use lower concentrations (2.5–5%) in skin of color.
Chemical Peels and Lasers
Can be highly effective but carry a higher risk of post-procedure PIH in darker skin if not used correctly. Seek practitioners with specific experience in skin of color.
Sunscreen
Non-negotiable. UV exposure is the single greatest factor prolonging PIH. Broad-spectrum SPF 30+ daily, even on cloudy days.
When seeking treatment, look for a Board-Certified Dermatologist with documented experience treating skin of color. Ask directly — it is a reasonable and important question, and the answer will shape the quality of your care.
Final Word
Acne is a biological process rooted in the pore. What it leaves behind — whether dark spots, redness, or structural scars — depends on the depth of inflammation, individual healing responses, and critically, skin tone. For people with darker skin, the aftermath is often the harder, longer battle.
Understanding this distinction is essential to having the right skin care. The good news: with the right treatment approach, timed early and tailored to your skin tone, both acne and its aftermath are highly manageable. Your skin tone should shape your treatment plan — it should never limit the quality of the care you receive.